Most parents think of giving any type of praise as an instant motivation boost. But that’s not always the case when it comes to children.
In fact, several studies have found that when teachers give feedback to students, they convey messages that affect the students’ opinions of themselves and how capable — or incapable — they are of academic achievement.
And as a child psychologist, I’ve found that certain types of praise can do more harm than good to a child’s independence, learning drive, self-confidence and resilience.
How praise impacts your child’s mindset
Carol Dweck, a psychologist and professor at Stanford University, has been studying the impact of praise on children for decades.
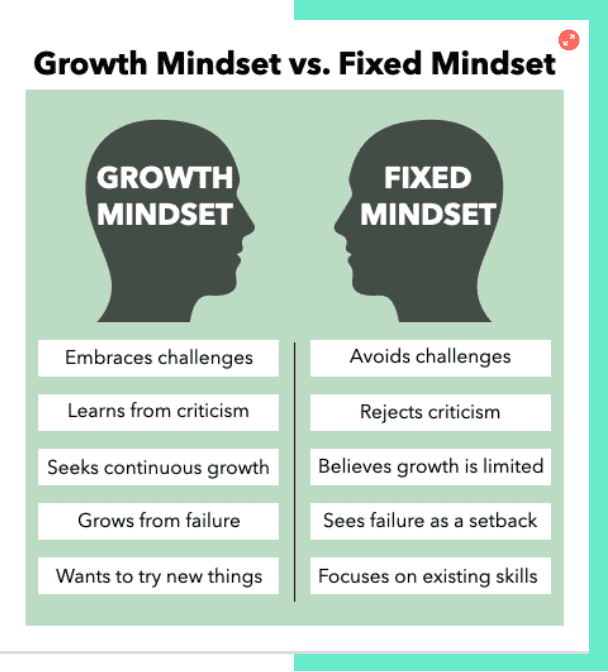
In her research, she identified two core mindsets — or beliefs — about one’s own traits. These mindsets shape how people approach challenges:
- Fixed mindset: The belief that one’s abilities are carved in stone and predetermined at birth.
- Growth mindset: The belief that one’s skills and qualities can be cultivated through effort and perseverance.
People with a fixed mindset, she found, tend to ignore feedback, give up easily and measure success by comparing themselves to others. In contrast, those with a growth mindset are more likely to embrace challenges and make self-to-self comparisons.
Focus more on praising the process, not the outcome
By praising the process (“I love how you were very thoughtful about the colors you chose!”), and not the outcome (“The colors in your drawing are beautiful! You’ve got a good eye.”), is what helps children develop a growth mindset, according to Dweck.
When parents praise the outcome, it holds kids back from developing resilience, confidence and a desire to learn new things.
Imagine two kids on a track team. The first kid is a passionate runner, while the second is less athletic. The kid who loves running exerts minimal effort at practice and still wins first place in almost every track meet. The second kid pushes himself, but is discouraged by the fact that he hasn’t had a win.
To praise the process, the parent of the natural runner should acknowledge her skill without providing excessive celebration or praise. This will help her feel supported without suggesting that her innate ability is the primary factor in determining her success.
The parents of the less athletic child should praise him for his hard work and perseverance. This helps him maintain his self-esteem and stay motivated to succeed.
Teach that failure creates opportunity
To further support your child’s development of a growth mindset, move your sole focus away from their accomplishments and steer the same level of attention towards their imperfections.
Encourage them to recognize, accept and overcome their “weaknesses.” Remind them that they have the tools and support to grow in the ways that they want to.
Let’s say your child failed his math test twice in a row. Instead of responding with “well, this is disappointing” or “you’re not studying hard enough,” react to his failure as though it’s something that can enhance his learning.
Talk through questions like: “What is this teaching us?” “What should we do next?” “Maybe we can talk to your teacher about how you can learn this better?” This way, your child can come to understand that abilities and skills are not limited; They can be cultivated, and doing so can be a fruitful and wonderful experience.
Children who value learning and effort know how to make and sustain a commitment to their goals. They are not afraid to work hard, and they know that meaningful tasks involve setbacks. These are the lessons that will serve them well in life.
Francyne Zeltser is a child psychologist, adjunct professor and mother of two. She promotes a supportive, problem-solving approach where her patients learn adaptive strategies to manage challenges and work toward achieving both short-term and long-term goals. Her work has been featured in NY Metro Parents and Parents.com.
Don’t miss:
- A psychotherapist says the most mentally strong kids always do these 7 things—and how parents can teach them
- Psychotherapist: Parents of mentally strong kids always do these 3 things when giving praise
- Why psychologists say ‘positive parenting’ is one of the best styles for raising strong, confident kids

Can you believe that we will all say goodbye to 2022 in less than 30 days? This year has certainly flown past us in a blink of an eye. Before every year ends, I like to meet with parents to review and reflect on how ABA therapy has helped their child since starting services. This also sets up the stage for what we can plan to work on for next year.
This year, I have had the pleasure of working with families that are relatively new to ABA. I interviewed four different families who are new to ABA therapy. The purpose of this interview was to: (1) lend continued support for ABA therapy as an evidence based practice for helping families and children with ASD, and (2) lend continued support for parent counseling and training (PCAT) as an essential component of ABA therapy.
Q1: Has your perspective of ABA therapy changed at all since you first learned about it? How?
Parent 1:
“Definitely has changed. Good change for the better. When I first learned about ABA, my first experience was hearing it from other people and parents who probably had a really bad prior experience with it. “ABA will make your child like a robot,” was one of the most shocking comments that I first heard about it. I disagree with those kinds of comments completely.
I feel that since my son has started receiving ABA therapy, it has been the most beneficial service out of everything else. Working with an experienced BCBA has helped me understand how basic behavior science can be applied to help me understand why my son is behaving or acting out a certain way. These experiences have also helped me become a better parent that now only wants to learn more.”
Q2: What do you hope to achieve with ABA therapy?
Parent 2:
“I hope that ABA therapy can help my son become more independent and make his own decisions in life. Even though my son cannot talk with his own voice due to his disability, I hope that one day that ABA can help him communicate not just his needs and wants, but maybe one day his thoughts and feelings. As his mother, you can’t help but wonder, “What is my son thinking?” or “How is my son really feeling?” I am his one and only voice at the moment, and I hope that ABA can help him give him more of that ability to be autonomous.”
Q3: What kind of traits do you think make up a good ABA therapist?
Parent 3:
“I think the traits that make up a good therapist are traits that my child and the therapist have in common. It is just basic human nature to be able to connect more with other people who you share common interests with. For example, my son loves video games, Pokemon, and Anime, which are all things that I have tried getting into, but I just do not know as much as his therapist does. Children love when adults like the same things that they do.
My son’s therapist acts almost like a “big brother” role model to him in this way. He is able to incorporate learning opportunities that occur naturally which is incredibly brilliant and a refreshing way to teach these important life skills to my son. For example, one day his therapist was able to teach my son an important lesson on self-regulation skills during a really big tantrum he was having. Within minutes, his therapist was able to help him self-regulate and take perspective of the situation by using a technique called Behavior Skills Training.
It really helps when the therapist is both experienced in working with children who are a lot like my son, and also just extremely patient, communicative, and friendly. There is a warm and comfortable feeling that develops over time, once you begin to realize how lucky you are to find a therapist that truly cares and understands him.”
Q4: How do you feel supported in therapy and any recommendations in ways that we can support better?
Parent 4:
“I feel very supported in my son’s ABA therapy. I really like how his therapist always takes the time to speak with me to tell me what goals he is working on with him, what things he is doing well with, and what things he is having a hard time with. Communication is such an important thing here, especially when I can’t exactly sit down with my 8 year old with limited language skills and ask him, “So what did you learn today with your teacher (Andrew)?” It means a lot when they (the therapists) arrange the time to come visit our family at home.
Lately, there have been some moments when I do not know what is the right thing to do when my son is having a meltdown. It has been such a blessing to have a BCBA who can see his behaviors happen with his own eyes and immediately be there to provide feedback, recommendations, and support so that I can learn how to handle it on my own next time. I think that other BCBAs should do the same in which that they just spend a good amount of time seeing how the child’s family operates outside of the normal session hours to see if there can be any other behavior supports that can help not only me and my child, but provide support to my family members that share the same home and also take care of my son.”
Final reflections
We’re continuing to try to listen to the autistic community and their families, to ensure that we’re providing services that are leaving a positive impact. We encourage other BCBAs to take a moment to talk to their families at the year’s end on their thoughts, as well?

We all want to raise intelligent, confident and successful kids. But where to begin? And what’s the best parenting style to go with?
Parenting styles fall under four main categories. It might be that you use one or more of these different styles at different times, depending on the situation and context.
Research tells us that authoritative parenting is ranked highly in a number of ways: Academic, social-emotional and behavioral. Similar to authoritarian parents, authoritative parents expect a lot from their children — but they expect even more from their own behavior.
What is authoritative parenting?
Authoritative parents are supportive and often in tune with their children’s needs. They guide their kids through open and honest discussions to teach values and reasoning.
Like authoritarian parents, they set limits and enforce standards. But unlike authoritarian parents, they’re much more nurturing.
Some common traits of authoritative parents:
- Responsive to their child’s emotional needs, while having high standards
- Communicate frequently and take into consideration their child’s thoughts, feelings and opinions
- Allow natural consequences to occur, but use those opportunities to help their child reflect and learn
- Foster independence and reasoning
- Highly involved in their child’s progress and growth
Why experts agree authoritative parenting is the most effective style
Studies have found that authoritative parents are more likely to raise confident kids who achieve academic success, have better social skills and are more capable at problem-solving.
Instead of always coming to their kid’s rescue, which is more typical among permissive parents, authoritative parents allow their kids to make mistakes. This offers kids the opportunity to learn while also letting them know that their parents will be there to support them.
Authoritative parenting is especially helpful when dealing with conflict, because the way we learn to deal with conflict at a young age plays a big role in how we handle our losses or how resilient we are in our adult lives.
With permissive parents, solutions to conflicts are generally up to the child. The child “wins” and the parent “loses.” I’ve seen this approach lead to kids becoming more self-centered and less able to self-regulate.
Of course, there are times when a punishment, like taking a time out, is necessary. But the problem with constant punishment is that it doesn’t actually teach your kid anything helpful. In most cases, it teaches them that the person with the most power wins, fair or not.
Let’s say your 10-year-old son begs not to go to soccer practice: “I don’t want to because I don’t think I’m good at it.”
In response,
- A permissive parent might say, “It’s up to you.”
- A neglectful parent might say, “Whatever you want … it’s your life.”
- An authoritarian parent might say, “You have to. I don’t want to hear another word from you.”
- An authoritative parent might say, “I understand that you don’t want to go. But sometimes, fighting the urge to avoid doing something hard is how you get better!”
While authoritative parents do set limits and expect their kids to behave responsibly, they don’t just demand blind obedience. They communicate and reason with the child, which can help inspire cooperation and teach kids the reason behind the rules.
Authoritative parenting doesn’t guarantee success
While experts give authoritative parenting the most praise, it’s important to note that using just one method does not always guarantee positive outcomes.
Parenting isn’t an exact science. In many ways, it’s more like an art. As a child psychologist and mother, my advice is to be loving and understanding — but to also create structure and boundaries.
Don’t simply focus on punishment. Be supportive and really listen to your child. Ask them questions and try to understand things from their point of view. Allow them into the decision-making process so that they can grow and learn things on their own.
There’s a difference between parenting styles and parenting practices. A parenting style is the emotional climate in which you raise your child, and a parenting practice is a specific action that parents employ in their parenting.
In short, behave as the good human you want them to be.
Francyne Zeltser is a child psychologist, adjunct professor and mother of two. She promotes a supportive, problem-solving approach where her patients learn adaptive strategies to manage challenges and work toward achieving both short-term and long-term goals. Her work has been featured in NYMetroParents.com and Parents.com.
Don’t miss:

The research and methodologies of Applied Behavior Analysis (ABA) have progressed and modernized drastically since its debut in the late 1960s. ABA is a scientific philosophy, and it is a way of understanding human behavior to be used to its advantage serving as an evidence based practice. Brilliant behavioral psychologists during these past few decades have been able to come together and develop revolutionary ways of teaching new skills and modifying behaviors.
What is DTT?
Discrete Trial Teaching (DTT) is a well-known ABA teaching procedure developed by Dr. Ivar Lovaas in the 1970s. DTT is a one-to-one instructional approach used to teach skills in a planned, controlled, and systematic manner in which the learner is taught a skill separated into small repeated steps (Bogin, 2008). For example, if you were teaching a child how to read sight words, you would teach the same set of five sight words over and over until essentially “perfection” and no errors are made after a specified amount of consecutive sessions. To some practitioners, DTT may be perceived as “rote” or “highly repetitive” because DTT is sometimes characterized as “intense” and “repetitive” in its methodology. The amassed practice and repetition of learning trials can be beneficial for younger children (typically between the ages of 2 and 9) for teaching simple receptive skills such as tacting (labeling) objects, identifying colors, or following one-step directions.
DTT Challenges
However, using DTT can be challenging for teaching more advanced older learners more complicated or skills that require many steps such as: vocational skills, conversational skills, self-care skills, and many more. Most developmental disabilities such as autism are considered a lifelong disability. Therefore, DTT may not be the most appropriate teaching strategy for older children, teens, adults, and beyond. Luckily, there are many other options to choose from.
NET: An Alternative to DTT
Well-trained and experienced behavior analysts are aware of the many other teaching alternatives to choose from other than DTT. When I am providing direct ABA services, I prefer to follow a much more natural and relaxed teaching style. Natural Environment Teaching (NET) is also an evidenced based practice in which ABA practitioners incorporate the learner’s natural environment into the teaching, development, and generalization of skills. These learning experiences are incorporated into play activities using familiar toys, games, and materials to maximize the learner’s motivation to continue the activity. With NET, the learner is essentially in control of their environment and they have full autonomy on which activities they choose to do.
NET In Everyday ABA Practice
To best describe how and why I prefer to use NET in my everyday practice, I will explain the case of one of my 10 year old clients. Today, he returned back home after a long day at school (also a very long bus ride home!) and was very tired and he wanted to watch some of his favorite YouTube videos together on his favorite spot on the living room couch. This is very understandable, as I also like to do the same thing after being trapped in NYC traffic during the home rush hour almost every night!
I am thankful that I have such a wonderful and close rapport with him as his therapist. It is my presence and involvement in watching the videos together that has been the ultimate reinforcer for him since we have met. This gives me a teaching advantage during these situations in which I am able to provide natural teaching opportunities based on whatever he is choosing to watch. For example, today I was able to practice his expressive communication skills with learning to say, “again please” (for when he wants to hear the song again), “stop please” (for when he wants the video stopped), and “help me” (for whenever he would come across a technical issue with the computer). Because all of these situations were not contrived and occurred naturally, the learning experience becomes even more rewarding and meaningful. This also makes these target behaviors more likely to occur again.
Benefits of NET over DTT
Children are more likely to experience natural reinforcement outside of their therapy sessions when learning opportunities are incorporated into environments that are familiar to them. It is not worthwhile for them to learn how to memorize answers or responses through rote methods like DTT which are monotonous and not fun for the child. This is especially true if the learning experiences they acquire are not socially significant and do not functionally apply to their everyday environment. NET as an ideal teaching strategy is one of the many other ways that it can prevail over DTT.
For more information about the comparison between DTT and NET, please refer to the following article: https://psycnet.apa.org/fulltext/2014-44014-007.html
References:
Bogin, J. (2008). Overview of discrete trial training. Sacramento, CA: National Professional Development Center on Autism Spectrum Disorders, M.I.N.D. Institute, The University of California at Davis Medical School.

It’s OK to feel sad it’s almost time for your kids to return to school, and/or relieved it’s almost time for your kids to return to school.
As families prepare to return to school in the coming weeks, here are some tips for success for a smooth transition from summer break:
1. Ease anxiety through familiarity: Tour the school or meet the teacher, and schedule a play date with a classmate or plan a carpool in advance. Preparing your child for a new school, classroom, and friendships and calm their concerns.
2. Don’t force your child to cram for class! Last minute academic prep can make a child feel like they did not prepare enough for school over the summer, and can heighten their feelings of anxiety. To get back into the swing of learning, try educational opportunities they enjoy, like reading, playing a board game, or working on a puzzle together.
3. Reset for your school routine: Ease back into your child’s morning wakeups and evening bedtime routine during the week before the first day of school. This will make the process a smoother transition for your child when school starts, and ensure they are well rested for it.
4. Talk through expectations: Discuss classes or extra-curricular activities your child will look forward to with them, in order to generate excitement over the return to school. But talk with them about classes or experiences they may not enjoy, as well, like a challenging subject or riding the bus. Talking through difficult emotions together can help them prepare for the more difficult events, and practice expressing their feelings for open communication with you through the school year.
It is natural for a child to begin a new school year with increased anxiety or changes in appetite, sleep habits, irritability, or other behaviors. If you do not notice them return to their “normal” selves after they have adjusted to their new school routine, however, or their anxiety, sadness, or emotions are disrupting their day-to-day life, we recommend you seek additional support from a professional.
For more information on our Special Group Programs or individual treatment options for children and teens, contact us.

ABA stands for Applied Behavioral Analysis. It refers to using scientific behavioral principles to manipulate a learner’s environment to help them gain skills quickly and effectively. ABA therapy, when done well, takes a unique approach to meet every learner’s specific needs, prioritizes caregivers’ goals and concerns, and flexes based on a family’s ability and/or willingness to implement treatment.
Punishment, as defined in the field of ABA, is simply something that happens after a behavior that reduces the likelihood of that behavior happening again. Punishment in these terms happens constantly in all our daily lives. For example, a few months ago I made my daughter slow roasted salmon over a citrus salad, and she told me it was “ahsgusting”. She effectively punished my behavior—I have not again made this meal for her dinner. In a therapeutic setting, it could mean taking away screen time if a child hits or giving a time-out if a learner begins throwing materials at their siblings.
Rules regarding punishment in ABA
Behavior Analysts have very strict rules about when and why to use punishment. For our earliest learners, punishment is only to be used after attempts at reinforcement have failed. An example would be we might offer a three-year-old a sticker for every five minutes they don’t throw hard objects. If this resolves the object-throwing behavior, there is no need for punishment. We would only consider punishment in this scenario because throwing hard objects can be dangerous to others in the child’s environment. For older learners, punishment might be used more hastily to quickly reduce dangerous behaviors—but always in conjunction with a reinforcement procedure. This could look like a 10-year-old getting a time out if he punches his brother but earning tokens to cash in for a larger prize for every 15 minutes, he has a safe body. In both cases, punishment is only being used because there is a present safety hazard.
Punishment, when implemented ethically and correctly, reduces dangerous behaviors in conjunction with reinforcement procedures. Historically, ABA providers have used punishment in other circumstances, such as to reduce stimming behaviors. As long as the stimming behavior does not present a danger or impediment to a child’s life, there is no need for the behavior to be reduced via punishment. Sometimes, stimming behaviors can be dangerous. For example, if a child is engaging in eye-stimming behavior while crossing the street, they may not see cars coming. An individual who likes to rub fabrics could get in real trouble if they start rubbing strangers on the street. Classic stimming behaviors like flapping or rocking may get in a learner’s way (it’s hard to learn to write or type when one is flapping), but this does not mean these behaviors need to be punished. Rather, finding appropriate times and places to engage in stimming behavior (changing when it happens as opposed to the fact that it does happen), is preferable to punishing something that a child clearly feels they need to do and is not harmful.
Evolving perspective on punishment in the field
This is a relatively new perspective for our field, and I am sure there are many neurodivergent individual today who were treated differently by ABA therapists in the past. Just like other fields, ABA is a constantly growing and evolving form of practice that constantly seeks to improve its ethical and practice standards. Similar to how the field of psychology has undergone similar evolutions from the ethical stumbles of the Zimbardo Prison Experiment, and The Milgram Shock Experiment, the field of ABA has been evolving since the days Ivar Lovaas tried to make children with ASD indistinguishable from their peers.
Ultimately, when ABA is being implemented properly, the impact of punishment is a reduction of the behavior that was being punished. Now, BCBAs may want to think long and hard about if and when punishment is going to be implemented. Providers may want to ask themselves, has my client or their parents expressly consented to this procedure? If not, the impact of the punishment may serve to reduce trust and faith with your client and their family, and our field overall.
A child psychologist explains a trending service: potty training consultations. Here’s what parents need to know about the specialists who are paid to provide guidance, coaching, and support through this milestone.
Young children learn new skills through interactions with their environment. Potty training is one of these skills—it is not innate and needs to be explicitly taught to most young children. Using the bathroom is a major transition for most toddlers who have spent their entire lives going in their diapers, anytime and anywhere. They now not only have to go in a potty, but they also have to identify the urge of having to go, hold ‘it’ in, communicate their need to go, and then make it to the potty in time.

Most potty training methods are grounded in behavioral psychology, which relies heavily on reinforcement to shape new behaviors. This process, called conditioning, is the foundation of most potty training strategies. While some children potty train themselves, most need to be prompted and supported by the adults, mostly parents or guardians, in their lives to fully transition from diapers to underwear.
While some parents find success in choosing a traditional potty training method, many others struggle to implement one consistently. This leaves them frustrated or overwhelmed when the process is harder or takes longer than expected. While most parents would not hesitate to hire a tutor to support their struggling student, they question whether hiring a potty training consultant is appropriate or necessary. But there is no shame in asking and paying for help in parenting when you can afford to.
This is where I come in. I’m a licensed child psychologist who specializes in cognitive and behavioral therapies. While I am not exclusively a professional potty trainer, I am a potty training expert and am often called in to provide consultation and support to families who struggle to potty train their children on their own. Here’s what I want parents to know:
What is a Potty Training Consultant?
Recently, more and more families are beginning to talk about their potty training struggles and are seeking help. Today, many parents are juggling the responsibilities of child-rearing with the pressures of full-time careers. The patience and consistency needed to effectively potty train are often overshadowed by the realities of modern life. Even parents who have the ability may not have the bandwidth to devote the time and resources needed while tending to multiple children or supporting various schedules or activities. Other times, parents have exhausted all their resources and are at their wits’ end. This is when they call in the expert.
A potty training consultant is an individual with extensive experience working with children who are resistant or difficult to potty train. Consultants often have a background in psychology, have received training in behavioral methods to support potty training, or completed a potty training certification course to help support their practice. Potty training consultants help you troubleshoot your potty training obstacles and get your child on the path to success. They work with parents to create a plan that works for them and their child to address issues they may be experiencing.
Potty Training Specialist Cost and Services
Potty training consultants offer a wide array of services from phone consultations to in-home potty training. Suggested services are based on the family’s needs. Phone consultation is usually the stepping stone for parents who are frustrated and overwhelmed with the potty training process and need a little extra hand-holding and support. These parents are either looking for a plan to get started or to troubleshoot and tweak what they are currently doing.
In-home potty training allows for demonstrations and hands-on coaching and support. In-home training is typically provided by the day with one to two days recommended depending on the child’s age and whether potty training has already been introduced. In some cases, a half-day is sufficient and in other cases, such as working with children with special needs, three or more days may be needed. Parents are expected to continue using the techniques and supporting the process after the consultant leaves.
Cost of services range based on where the consultant and family reside and what the fair market value is in that region with phone consultations being the more affordable option. In-home training rates range from $50 to $300 an hour based on total time reserved, the consultant’s credentials, and the specifics of the training case. Consultants may charge additional fees when traveling outside of their region.
Potty Training Consultant Vs. Potty Training Classes
Potty training consultants work one-on-one with your family to meet your specific potty training goals. Potty training schools offer group classes for parents or memberships that help support families throughout the potty training process. Each school offers different classes and levels of support, but like many other group supports, such as SAT prep classes and schools, the one-size-fits-all method to potty training does not actually fit all children.”Like teaching anything else, the approach to potty training should be individualized for each child,” says Samantha Allen, professional potty trainer and a behavioral specialist at NYC Potty Training. “If a child exhibits resistance or anxiety about using the toilet, it’s important to assess the underlying issue to help the child with that specific challenge.” Allen also noted a drawback of training schools: no one wants to poop with an audience.
Should I Hire a Professional Potty Trainer?
“Potty training can be extremely stressful and anxiety-inducing for many parents,” explains Kimberly Walker, pediatric sleep therapist and potty training consultant at Parenting Unlimited. “Often, they feel lost on where and how to start and this confusion transfers to the child creating a chaotic, negative experience for everyone.”
This is why hiring a consultant can be helpful. Potty training specialists help remove any power struggle from the experience. They can also cater services for a child who has special needs and may need alternative training methods implemented. A professional keeps parents involved in the training, without making it all-encompassing for them. That, says Allen, is one of the keys to successful potty training.
Finding a Potty Training Consultant Near You
Outsourcing potty training is more common in metropolitan areas says Lauren Trotter, a mom to a 4-year-old son in Houston, Texas. Trotter did a Google search to find a potty training consultant in her area. “The truth is, I didn’t even know where to start,” she says. “And this may not be the case for every family, but I really felt that potty training fell solely on my already hectic plate of things to do as a working mom; it’s completely unfair.” Perhaps one of the silver linings of the COVID-19 pandemic is the increase in accessibility and the ability to communicate virtually, so Trotter ended up contacting me, a NY-based potty training consultant, for support.
Trotter and I worked together to develop a strategy to train her son. “For me, getting professional help was the best decision I ever made,” says Trotter. “I was expecting to learn a lot from hiring a consultant but what I didn’t realize was how much I needed support, counseling, and the encouragement to hold my son’s daycare, my son, and myself accountable.”
If you are interested in finding a potty training consultant, a great place to start is by searching for professional potty training services in your area on Google. Read more about when to start potty training here.
Francyne Zeltser is a licensed psychologist, certified school psychologist, adjunct professor, and mom of two in New York. Dr. Zeltser promotes a supportive, problem-solving approach where her clients learn adaptive strategies to manage challenges and work toward achieving both short-and-long-term goals. You can connect by email, DoctorZeltser@gmail.com.
 Trauma can be difficult to define since each individual experiences and processes life events and trauma differently. Trauma can include abuse, neglect, domestic violence in the family, exposure to substance abuse, or divorce. Children with developmental disabilities are statistically at a higher risk to experiencing trauma than their typically developing peers (Rajamaran et al., 2022).
Trauma can be difficult to define since each individual experiences and processes life events and trauma differently. Trauma can include abuse, neglect, domestic violence in the family, exposure to substance abuse, or divorce. Children with developmental disabilities are statistically at a higher risk to experiencing trauma than their typically developing peers (Rajamaran et al., 2022).
Evidence shows that trauma may impact the physiological and behavioral development of a child (Teicher et al., 2016) and therefore affect one’s response to environmental scenarios. For example, conducting all components of a traditional functional analysis for a child who has experienced neglect would be unethical and harmful (Ramajaran et al., 2022). In other words, imagine not being “informed” or not “assuming” trauma, and thereby placing a child in a room where they are meant to feel alone, for the sole purpose of identifying the function of a given behavior to be automatically reinforcing.
Trauma-Informed Care vs. Trauma-Assumed Care
Trauma-informed care suggests that the provider is aware of trauma experienced by the client, however we aren’t always notified of these events for many potential reasons. Trauma-assumed care is a proactive way of treating our clients, since statistics show that most adults have experienced at least one adverse childhood experience in their lifetime (ACEs; Felitti et al., 1998). We may not be informed of the trauma our clients have experienced during pre-analysis interviews, and it is unlikely that we observe the direct contingencies during these traumatic events. Behavior analysts must know that the impact of trauma has long-term effects on an individual’s psychological and behavioral health, and this should affect the way we teach and treat our clients.
Why is Everyone Talking About Trauma-Assumed Care Now? Recent research is directing behavior analysts to be mindful of their client’s past and to account for trauma when treatment planning and assessing. It is our ethical duty to include TIC in ABA because without doing so, we could be compromising our reputation as behavior analysts, as well as the effectiveness of the treatment we provide (Rajamaran et al., 2022).
A Clarification of Trauma-Assumed Care:
Trauma- assumed care in ABA is a proactive approach to intervention, accounting for the individual’s potential exposure to trauma. It means providing a therapeutic experience that is sensitive to the probability of trauma. This is different from “trauma-specific service,” in which the objective is to directly treat an individual for the trauma that they have experienced (DeCandia et al., 2014). It is our duty to “acknowledge trauma and its potential impact” (Ramajaran et al., 2022) when treating our clients.
Trauma’s Impact on Care
First, it is important that we are aware of where trauma comes from and that we may not ever know about the trauma that a child has experienced. For one, the odds increase that an individual with an intellectual or cognitive disability faces adverse childhood experiences (ACE) in their lifetime (McDonnell et al., 2019). Most of us are treating children on the spectrum or with other disabilities who have experienced trauma, but don’t have a way of describing and communicating that (McDonnell et al., 2019; Ramajaran et al., 2022).
A child engaging in severe or undesired behavior may be “adapting to and coping with past traumatic experiences” (Guarino et al., 2009; Ramajaran et al., 2022). A true behavior analyst understands that stimulus-stimulus pairing could have occurred between a traumatic event and another neutral stimulus. For example, if a child experienced physical abuse,undesirable behaviors could occur in the presence of adults who utilize physical or proximity prompts. (Ramajaran et al., 2002). As another example, it may be insensitive to utilize a response cost system with a child who was in foster care or who has lost a loved one. It’s important to know your learner and their history when assessing and treatment planning to first “do no harm” and to secondly, provide positive meaningful outcomes.
Choice in Trauma-Assumed Care
Secondly, providing an individual with choices has been one evidence-based practice as well as our ethical duty to promote socially valid treatment (BACB, 2020; DeCandia et al., 2014). The professional is providing the individual with a choice to not experience a potentially traumatizing stimulus or event, and instead involves the client in setting their goals, and with making decisions. Hanley (2010) has outlined a few ways to provide choices regarding the procedures and outcomes of an intervention for individuals who are less verbal. One approach includes using a concurrent operant preference assessment. Brower-Breitweisre (2008) gave autistic children the choice to learn through Applied Behavior Analysis (ABA) or Treatment and Education of Autistic and Communication Handicapped Children (TEACCH) through a concurrent operant preference assessment. Providing an individual with choices is crucial if we are concerned with one’s quality of life (Martin et al., 2006).
Trauma- Assumed Care and Assent:
In today’s ABA (Hanley, 2019), we worry about the child assenting to the procedures and the outcomes. Hanley instructs all BCBA’s to find the child’s state of happiness, relaxation, and engagement before demands are presented (2019). To acknowledge that trauma has occurred, we respond to noncompliance and aggressions with functional communication training and skill based treatments, by avoiding the overuse of extinction, and by keeping an open door policy so that individuals don’t feel threatened or forced to participate (Hanley, 2019). Trauma-assumed care is televisable, meaning that anyone watching would feel comfortable and sure that the individual in treatment is choosing to be there and is learning skills that improve their quality of life.
The theory that “the student is always right” also means that behavior should inform our decision making with the implementation of interventions (Keller, 1968). A child whose dangerous or maladaptive behavior continues to occur, isn’t learning the necessary replacement skills. Severe behaviors are a sign that there are communication and tolerance skills that are more socially significant than the skills that the child is likely to be avoiding and escaping. When a child is happy, relaxed, and engaged, the child has access to all reinforcers, including attention from adults and tangible reinforcers. Hanley (2019) encourages us to “forget the function” and treat maladaptive behavior as a skill deficit for communication and tolerance. By teaching pivotal skills such as omnibus mands, toleration of transitions and denial of reinforcers, we reveal opportunities for the child to learn in a safe environment (Ward et al., 2020).
References (not complete)
Martin TL, Yu CT, Martin GL, Fazzio D. On Choice, Preference, and Preference for Choice. Behav Anal Today. 2006;7(2):234-241. doi: 10.1037/h0100083. PMID: 23372459; PMCID: PMC3558524.

If the question ″What type of parent do I want to be?” has ever crossed your mind, it helps to understand the basics of different parenting styles.
The 4 types of parenting
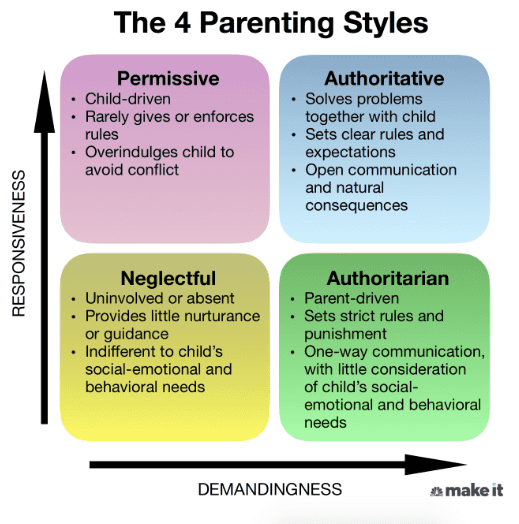
The four main parenting styles — permissive, authoritative, neglectful and authoritarian — used in child psychology today are based on the work of Diana Baumrind, a developmental psychologist, and Stanford researchers Eleanor Maccoby and John Martin.
Each parenting style has different effects on children’s behavior and can be identified by certain characteristics, as well as degrees of responsiveness (the extent to which parents are warm and sensitive to their children’s needs) and demandingness (the extent of control parents put on their children in an attempt to influence their behavior).
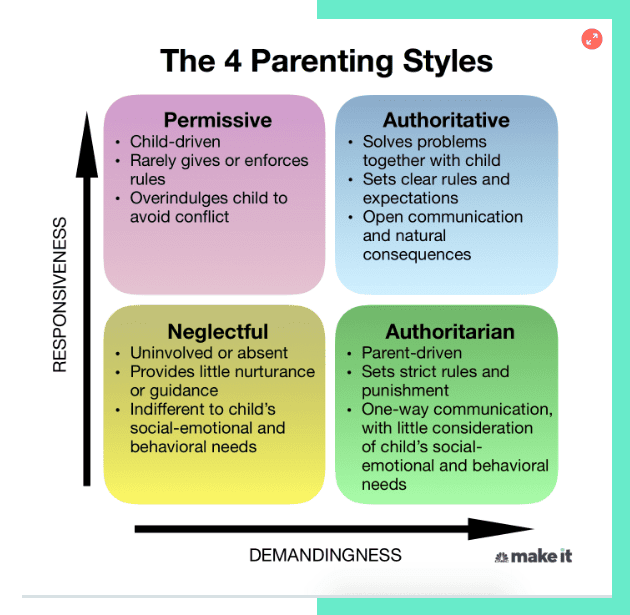
1. The Permissive Parent
Common traits:
- High responsiveness, low demandingness
- Communicates openly and usually lets their kids decide for themselves, rather than giving direction
- Rules and expectations are either not set or rarely enforced
- Typically goes through great lengths to keep their kids happy, sometimes at their own expense
Permissive parents are more likely to take on a friendship role, rather than a parenting role, with their kids. They prefer to avoid conflict and will often acquiesce to their children’s pleas at the first sign of distress. These parents mostly allow their kids to do what they want and offer limited guidance or direction.
2. The Authoritative Parent
Common traits:
- High responsiveness, high demandingness
- Sets clear rules and expectations for their kids while practicing flexibility and understanding
- Communicates frequently; they listen to and take into consideration their children’s thoughts, feelings and opinions
- Allows natural consequences to occur (e.g., kid fails quiz when they didn’t study), but uses those opportunities to help their kids reflect and learn
Authoritative parents are nurturing, supportive and often in tune with their children’s needs. They guide their children through open and honest discussions to teach values and reasoning. Kids who have authoritative parents tend to be self-disciplined and can think for themselves.
3. The Neglectful Parent
Common traits:
- Low responsiveness, low demandingness
- Lets their kids mostly fend for themselves, perhaps because they are indifferent to their needs or are uninvolved/overwhelmed with other things
- Offers little nurturance, guidance and attention
- Often struggles with their own self-esteem issues and has a hard time forming close relationships
Sometimes referred to as uninvolved parenting, this style is exemplified by an overall sense of indifference. Neglectful parents have limited engagement with their children and rarely implement rules. They can also be seen as cold and uncaring — but not always intentionally, as they are often struggling with their own issues.
4. The Authoritarian Parent
Common traits:
- High demandingness, low responsiveness
- Enforces strict rules with little consideration of their kid’s feelings or social-emotional and behavioral needs
- Often says “because I said so” when their kid questions the reasons behind a rule or consequence
- Communication is mostly one-way — from parent to child
This rigid parenting style uses stern discipline, often justified as “tough love.” In attempt to be in full control, authoritarian parents often talk to their children without wanting input or feedback.
What is the best parenting style for you?
Research suggests that authoritative parents are more likely to raise independent, self-reliant and socially competent kids.
While children of authoritative parents are not immune to mental health issues, relationship difficulties, substance abuse, poor self-regulation or low self-esteem, these traits are more commonly seen in children of parents who strictly employ authoritarian, permissive or uninvolved parenting styles.
Of course, when it comes to parenting, there is no “one size fits all.” You don’t need to subscribe to just one type, as there may be times when you have to use a varied parenting approach — but in moderation.
The most successful parents know when to change their style, depending on the situation. An authoritative parent, for example, may want to become more permissive when a child is ill, by continuing to provide warmth and letting go of some control (e.g. “Sure, you can have some ice cream for lunch and dinner.”).
And a permissive parent may be more strict if a child’s safety is at stake, like when crossing a busy street (e.g. “You’re going to hold my hand whether you like it or not.”).
At the end of the day, use your best judgement and remember that the parenting style that works best for your family at that time is the one you should use.
Francyne Zeltser is a child psychologist, school psychologist, adjunct professor and mother of two. She promotes a supportive, problem-solving approach where her patients learn adaptive strategies to manage challenges and work toward achieving both short-term and long-term goals. Her work has been featured in NYMetroParents.com and Parents.com.
Don’t miss:
- A psychotherapist says the most mentally strong kids always do these 7 things—and how parents can teach them
- I raised 2 successful CEOs and a doctor. Here’s one of the biggest mistakes I see parents making
- A psychologist shares the 5 phrases parents should never say to their kids—and what to use instead

When is there consent?
Consent occurs when an individual, typically a parent or guardian, legally permits another individual’s participation. Consent is typically obtained through spoken and written authorization. Assent, on the other hand, is a non-legally binding agreement to participate in an intervention, provided by the client themself. Assent is obtained usually by a child or a dependent adult who cannot make legal decisions for themselves. Acquiring assent from a client may occur in spoken or written communication, but can also differ based on the language and cognitive abilities of that individual.
Why is assent important, if we already are obtaining legal authorization, or consent, from a legal guardian? Behavior Analysts have an ethical duty to acknowledge “…personal choice in service delivery…by providing clients and stakeholders with needed information to make informed choices about services” (BACB, 2020, p.4). Making an effort to obtain assent is how we keep client dignity and provide trauma-assumed care. According to the Federal Policy for the Protection of Human Subjects (FPPHS), it is not legally required to obtain assent from children prior to proceeding with interventions (2008). However, according to the Behavior Analyst Certification Board Code of Ethics (BACB), it is our responsibility to treat all individuals equally regardless of disability and age and to “acknowledge that personal choice in service delivery is important” (2020, p. 4). There are a lot of choices that professionals make when designing a behavioral plan. Prioritizing social validity in our practice includes seeking assent when choosing goals, procedures, and the results of the intervention (Wolf, 1978). There are many evidence based approaches for obtaining assent with young children and those with developmental disabilities.
What does assent look like?
Acquiring assent can look differently, depending on the individual one works with. With older children or children with advanced language abilities, one might simply ask the child if they would like to participate. One might also put an agreement in writing for the child, however there are several strategies that can be used with young children or language impaired individuals to acquire assent (Morris, Detrick & Peterson, 2021). Rapport building and instructional fading is one evidence based approach to increase a client’s voluntary participation (Shillingsburg, Hansen, & Wright, 2019). The implementer systematically fades from child-led play to an intensive teaching model across various phases. Instructional fading has shown to decrease problem avoidance maintained behavior, and increase longer durations of time of the child in close proximity to the therapist and in one’s seat without needing many additional resources (2019). In addition, BCBAs may find it simpler to train novice therapists and parents to utilize an instructional fading approach.
Morris et al. (2021) suggests the presentation of choices as another strategy to increase client voluntary participation and thereby accounting for assent. We should “respect and actively promote our client’s self-determination” and acknowledge the importance of our client’s choice during service delivery (BACB, 2020, p. 4). Instead of incorporating aversive interventions such as punishment and extinction to decrease problem behavior, try accounting for the child’s preference by offering choices. McComas (1996) allowed children to choose between emitting a maladaptive response versus utilizing functional communication in order to get access to a reinforcer, such as attention from an adult. By manipulating the duration of time allowed with the reinforcer and the quality of the reinforcer, one can teach children to prefer to use a more adaptive form of communication and to choose against emitting the maladaptive behavioral response. The children were provided access to a preferred stimulus for longer durations when emitting a functional communication response, and less time when emitting maladaptive behavior.
Utilizing concurrent chain procedures is one more way to account for the child’s preference of intervention procedures. By allowing the child to choose the treatment procedures, we are likely to see positive results, lower rates of problem behavior, and our practice remains socially valid. Torellii et al. (2016) conducted preference assessments to assess which topography children preferred when manding. Based on the child’s increased mand responses with the iPad®, it was decided that the child would utilize the iPad® for communication instead of the GoTalk® device. Other studies present how to utilize a concurrent chain procedure to examine client preference to using a microswitch, PECs, sign language, vocal speech and assistive technology device for manding (Winborn, Wacker, Richman, Asmus, & Geier, 2002; Winborn-Kemmerer, Ringdahl, Wacker, & Kitsukawa, 2009). For example, the instructor teaches the child two different mand topographies and then provides simultaneous access to both types of responses. The choice that the child makes when both options are available teaches the instructor which response type is preferred, thereby accounting for assent in procedures and results of the intervention.
How to approach assent and assent withdrawal
How often should we give choices to our clients and how can we account for assent withdrawal? There isn’t a one size fits all response, but it’s better to follow the rule of “the learner is always right” (Keller, 1968). Hanley (2021) encourages choice making and encourages professionals to listen to the child and attend to behaviors, even when we feel like it would be best to ignore those attention seeking behaviors. He also encourages all professionals to keep an open door because “leaving means something is missing or something aversive is present” (2021). By reducing physical behavioral management, and allowing freedom to move and choose where one prefers to be, we are allowing children to consent to the intervention. Rajamaran et al. (2020) gave the ongoing choice for children to either go to the instructional room, a “hangout room” with free access to preferred items and adult attention, or to go home. These children were selected because they exhibited dangerous problem behavior in order to escape or avoid demands and to get access to what they wanted. The results from this study showed that all three children chose to stay and learn important life skills such as functional communication, toleration responses, and contextually appropriate behavior (CAB) (2020) over 90% of the time and did not choose to go home (Rajamaran et al., 2021).
When given a choice between taking a break, or completing work, research has shown that children will choose to work in order to receive a longer or better break than receiving shorter breaks for “free” (Peterson et al., 2005). Children are more likely to stay engaged with a work task without problem behavior when the choice to not work is just as accessible. According to the matching law, individuals will choose to engage in more than one response type, based on the proportion of the reinforcement delivered for each response. Replacing problem behavior that includes partial extinction procedures encourages adaptive behavior through the delivery of higher levels of reinforcement for such positive behavior and lower levels of reinforcement for negative behavior. Many researchers such as Peterson et al. (2005) and Rajamaran et al. (2021) have shown how considering the child’s preference in participation has resulted in a decrease in problem behavior and an increase in children choosing to engage in learning tasks.
References
Behavior Analyst Certification Board. (2014). Professional and ethical compliance code for behavior analysts. Littleton, CO: Author.
Keller FS. “Good-bye, teacher…”. J Appl Behav Anal. 1968 Spring;1(1):79-89. doi: 10.1901/jaba.1968.1-79. PMID: 16795164; PMCID: PMC1310979.
Morris, C., Detrick, J.J. and Peterson, S.M. (2021), Participant assent in behavior analytic research: Considerations for participants with autism and developmental disabilities. Journal of Applied Behavior Analysis, 54: 1300-1316. https://doi.org/10.1002/jaba.859
Peterson, Stephanie & Caniglia, Cyndi & Royster, Amy & Macfarlane, Emily & Plowman, Kristen & Baird, Sally & Wu, Nadia. (2005). Blending functional communication training and choice making to improve task engagement and decrease problem behaviour. Educational Psychology – EDUC PSYCHOL-UK. 25. 257-274. 10.1080/0144341042000301193.
Rajaraman, A., Hanley, G. P., Gover, H. C., Staubitz, J. L., Staubitz, J. E., Simcoe, K. M., & Metras, R. (2022). Minimizing escalation by treating dangerous problem behavior within an enhanced choice model. Behavior Analysis in Practice, 15(1), 219–242. https://doi.org/10.1007/s40617-020-00548-2
Shillingsburg, M. A., Hansen, B., & Wright, M. (2019). Rapport Building and Instructional Fading Prior to Discrete Trial Instruction: Moving From Child-Led Play to Intensive Teaching. Behavior modification, 43(2), 288–306. https://doi.org/10.1177/0145445517751436
Winborn-Kemmerer L, Ringdahl JE, Wacker DP, Kitsukawa K. A demonstration of individual preference for novel mands during functional communication training. Journal of Applied Behavior Analysis. 2009;42:185–189.
Winborn L, Wacker DP, Richman DM, Asmus J, Geier D. Assessment of mand selection for functional communication training packages. Journal of Applied Behavior Analysis. 2002;35:295–298.
Wolf MM. Social validity: the case for subjective measurement or how applied behavior analysis is finding its heart. J Appl Behav Anal. 1978 Summer;11(2):203-14. doi: 10.1901/jaba.1978.11-203.